Please activate JavaScript!
Please install Adobe Flash Player, click here for download
ePaper created 2016-06-17, 09:51:15 | version 1.38.0
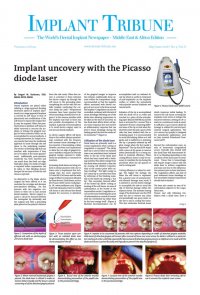
THE NINTH ANNUAL AMERICAN ACADEMY OF IMPLANT DENTISTRY MaxiCourse®- UAE 2016 – 2017 Starts August 30 A UNIQUE OPPORTUNITY DENTAL IMPLANTOLOGY In Fulfillment of the Educational Requirement for the Examination for Associate Fellow Membership for the American Academy Program Includes placement of 10 Implants with all surgical and prosthetic components, all materials for hands – on workshop and lecture handouts plus one complete surgical instrument Kit. MaxiCourse ® Advantage: 300 hours of comprehensive lectures, live surgeries, demonstration and hands-on sessions. In depth review of surgical and prosthetic protocols. Sessions stretch across 10 months in 5 modules of 6 days. Each session is always inclusive of a weekend. Over 15 speakers from the International Community who are amongst the most distinguished names in implantology will teach the curriculum. Certificate of completion awarded by the American Academy of Implant Dentistry. Non commercial, non sponsored course covering a wide spectrum of implant types and system. Hands-on patient treatment under direct AAID faculty supervision. Membership for AAID awarded for 2016 – 2017 Dates: Module 1 August 30th – September 4th 2016 Module 2 November 3rd – 8th 2016 Module 3 February 2nd – 7th 2017 Module 4 April 26th – May 1st 2017 Module 5 Dates to be announced Registration : Pre-Registration is Mandatory as it is a limited Participation Program. For further information and registration details visit website: www.maxicourseasia.com or e-mail Dr. Ninette Banday, Coordinator AAID-MaxiCourse UAE at drnbanday@yahoo.com The Faculty are as follows: Dr. Shankar Iyer, USA Director, AAID Maxi Course®UAE Diplomate AAID Clinical Assistant Professor,Rutgers School of Dental Medicine. Dr. Ninette Banday, UAE Co-Director AAID Maxicourse- Abu Dhabi, UAE Academic Associate Fellow AAID Dr. Amit Vora, USA Diplomate of the American Board of Periodontology Professor (partime) ,JFK Hospital and the Veteran Affairs (V.A.) Hospital Dr. Jaime Lozada, USA Director of the Graduate Program in Implant Dentistry Fellow, American Academy of Implant Dentistry Dr. William Locante, USA Diplomate of ABOI Fellow of American Academy of Implant Dentistry Dr. Robert Horowitz, USA Diplomate American Board of Periodontology Clinical Assistant Professor New York University Dr. Frank LaMar, USA Fellow, American Academy of Implant Dentistry Diplomate, American Board of Oral Implantology Dr. John Minichetti, USA Diplomat, American Board of Oral Implantology Honored Fellow, American Academy of Implant Dentistry Dr. Robert Schroering, USA Board Certified by the American Board of Oral Implantology Fellow, American Academy of Implant Dentistry Dr. Kim Gowey, USA Past President – AAID Diplomate ABOI Dr.Burnee Dunson, USA Fellow, American Academy of Implant Dentistry Diplomate ABOI Dr. Ahmed Ibrahim Osman UAE Director of Implant Center, University of Sharjah. Assistant Director of University Dental Hospital. Dr. Stuart Orton-Jones, UK Founder Member, The Pankey Association Member, Alabama Implant Study Group Director, The Stuart Orton-Jones Institute Dr. Robert Miller, USA Board Certified by the American Board of Oral Implantology/Implant Dentistry Honored Fellow American Academy of Implant Dentistry Dr. Philip Tardeu, France Founder and Author, Computer Guided Implantology and the Safe System. Dr. Natalie Wong, Canada Diplomate, American Board of Oral Implantology Fellow, American Academy of Implant Dentistry Dr. Irfan Kanchwala, India Implant Fellowship ( UMDNJ, USA) Diplomate , American Board of Prosthodontics Dr. Jason Kim, USA Diplomate of ABOI Eighth Annual Program Accredition by Health Authority Abu Dhabi for 252.75 CME Hours. Accredition for the Ninth Annual Program under process both with DHA & HAAD. Dental Tribune Middle East & Africa Edition | 3/2016 IMPLANT TRIBUNE 2 Figure9.Uncoveryof theimplantsandhealingscrewsexposed. Figure10.Healingabutmentsplacedinto theimplants. Figure 11. Removal of the healing abutments at 2 weeks post uncoverydemonstratingalackofinflammationof themodified soft tissue. biostimulatory effect that provides faster or more favorable wound healing, compared to tissue treated with a scalpel or electrosurgical unit. The laser irradiation stimulates the proliferation of mesenchymal stem cells without DNA alterations in the affected cells.13 Thus, wound healing is enhanced and soft tissue at the cut edges demonstrates faster heal- ing then when treated with a scalpel or other methods by stimulation of gingival fibroblasts inducing growth factors.14, 15 It has been reported that biostimulation via the diode laser also has a positive effect on bone cells and can be stimulatory to the bone cells at the crest around the implant.16, 17 Compared to conven- tionalmethodstissuehealingaswell as postoperative sensitivity was less with the diode laser then with other methods.18 Implant Uncovery technical considerations The width of attached gingiva re- mainingwilldictatethebestmethod for implant uncovery. (Figure 4A) When a wide band of attached gingi- vaispresentandasufficientamount (3mmorgreater)willbepresentafter uncoveryonboththebuccalandlin- gual then the diode laser is activated and inserted at the center of the site and worked in a spiral pattern out- ward until the entire cover screw is exposed. (Figure 4B) A curette or other instrument may be necessary to loosen the tissue over the cover screw as the periosteum during implant healing becomes adherent to the titanium cover screw. Sites that present with a narrow width of attached gingiva of 3-5mm at the crests center will require some con- servation of the remaining attached gingiva. In this clinical situation, the diode is utilized to remove an ellipti- cal piece of soft tissue over the cover screw and then the tissue is pushed buccally and lingually to preserve the attached gingiva. (Figure 4C) If less attached gingiva is present on either side of the center of the crest then the practitioner will need to preserve all of the attached gingiva present and a conventional flap is recommended to be able to position the tissue in a more apical direction. When this is necessary incisions can be made with the diode laser as an alternativetoascalpel.(Figure5) Casereport A30yearoldfemalepatientpresent- edwithseverelymalposedmaxillary central incisors tipped facially and a desire for esthetic improvement. A CBCT was taken and noted mini- mal bone was present over the facial of the central incisors. Options for treatment were presented to the pa- tient which included: orthodontics to correct esthetics or extraction of thecentralincisors,placementofim- plants at these sites and restorations ontheanteriorteeth. Thepatientin- dicated that she did not wish to pur- sue a orthodontic treatment option duetothetimeinvolved. The patient presented for surgery and the central incisors were atrau- matically extracted under local an- esthetic. The adjacent teeth were prepared for crowns, which would support a provisional bridge dur- ing the healing/integration period. A 4mm wide 24 degree Co-Axis im- plant (Keystone Dental, Burlington, MA) was placed into the osteotomy at each central incisor orienting the prosthetic axis to a vertical position while the implants body followed the trajectory of the premaxilla. A healing screw was placed and osse- ous graft material (NovaBone, Jack- sonville, FL) placed on the facial to thicken the resulting bone. The soft tissue was closed with resorbable PGA sutures. A stent created over the wax-up of the study models that hadbeenmodifiedwasfilledwithan auto-cure provisional resin (Perfect- emp 10, DenMat, Lompoc, CA) and seated over the anterior and allowed to set. Upon setting the stent with provisional was removed intraorally and trimmed and polished. The ma- terialattheimplantsiteswasshaped to a bullet shape to assist in forming an emergence profile in the soft tis- sueandpreservethepapilla’s. Six months post implant placement the provisional bridge was removed and preservation of the papilla’s was confirmed with a natural emergence profile within soft tissue. (Figure 6, 7) Local anesthetic was administered. The Picasso diode laser was set at 2.5 watts in continuous mode with an initiated tip and at the center of the depression in the soft tissue above the implants cover screw and moved in a circular motion moving outward until the entire cover screw was exposed. (Figure 8) The process cuts the desired soft tissue and co- agulates any bleeding from the cut edges. This was then repeated on the second implant. (Figure 9) Open tray implant impression abutments were placed into the implants and seating verified radiographically. An impressionofthemaxillaryarchwas taken utilizing Aquasil heavy body VPS(Caulk,Milford,DE)inaMiraAd- vanced Implant tray (Hager World- wide, Hickory, NC) and Aquasil Ultra syringed around the preparations and implant abutment heads. Heal- ing abutments were placed into the implants. (Figure 10) The previously placed provisional bridge was tried in and modified at the pontics to al- low the bridge to fully seat over the healing abutments and luted with a provisional cement (Fuji Temp LT, GCAmerica,Alsip,IL). Two weeks later the prosthetics re- turned from the lab (DenMat Labs, Lompoc, CA) and the provisional bridge was removed. The healing abutments were removed and the soft tissue demonstrated a lack of in- flammation and a good periodontal health where it had been modified by the diode laser. (Figure 11) Ceram- ic crowns were tried in on teeth 7, 10 and 11 and the screw retained zirco- nia based implant crowns inserted. A radiograph was taken verifying fit of the implant prosthetics. A torque wrench was utilized to tighten the fixationscrewsontheimplantsto30 Ncm and the ceramic crowns were luted with Panavia SA resin cement (Kuraray, NY, NY). Occlusion was checkedandadjustedwhereneeded. Conclusion: Diode lasers are a useful adjunct to soft tissue modification to uncover dental implants or esthetically re- contour the gingival margin. They provide better safety then electro surgery maintaining a temperature profile within the safety zone of bone and do not cause tissue shrink- age that can affect the esthetic out- come. As the diodes tip provides simultaneous cutting and coagula- tion (hemostasis) a clear advantage totheuseofascalpelortissuepunch immediate impressions can be ac- complished without site bleeding af- fectingtheaccuracyofthecaptureof thesofttissuecontoursandposition. References 1. Zetz MR, Quereshy FA.: Single- stage implant surgery using a tissue punch. J Oral Maxillofac Surg. 2000 Apr;58(4):456-7. 2. Wilcox CW, Wilwerding TM, Wat- son P, Morris JT.: Use of electro sur- gery and lasers in the presence of dental implants. Int J Oral Maxillofac Implants.2001Jul-Aug;16(4):578-82. 3. Goharkhay, K., Moritz, A., Wilder- Smith, P., Schoop, U., Kluger, W., Ja- kolitsch, S., & Sperr, W. (1999, June). Effects on Oral Soft Tissue Produced by a Diode Laser in Vitro. Lasers in SurgeryandMedicine,401–406. 4. Gherlone, EF. Maiorana C Grrani, .RF. Ciacaglini, R. Cattoni F. The use of an 980-nm Diode and 1064·nm Nd:YAG Liaser for Gingival Retrac- tion in Fixed Prosthsis/ Oral Laser Applications2004;4:183-190 The full list of references is available fromthepublisher. Dr.Kurtzman He is in private general practice in Silver Spring, Maryland and a former Assistant Clinical Professor at University of Maryland and a former AAID Im- plant Maxi-Course. He is aslo assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of Restorative dentistry, Endodon- tics and Implant surgery and prosthetics, removable and fixed prosthetics, Peri- odontics and has over 460 published arti- cles.HehasearnedFellowshipin theAGD, ACD, ICOI, Pierre Fauchard, ADI, Master- ship in the AGD and ICOI and Diplomat status in the ICOI and American Dental Implant Association(ADIA). Dr.Kurtzman has been honored to be included in the “Top Leaders in Continuing Education”by Dentistry Today annually since 2006 and wasfeaturedontheirJune2012cover. He can be reached at dr_kurtzman@mary- land-implants.com